Peer-reviewed publication
Publication: Critical Care Nursing Quarterly
Publication Reference: 2018 Jan/Mar;41(1):60-67
Authors: Diana C. Anderson, Ashley A. Jackson, Neil A. Halpern
Abstract
 Advanced informatics systems can help improve health care delivery and the environment of care for critically ill patients. However, identifying, testing, and deploying advanced informatics systems can be quite challenging. These processes often require involvement from a collaborative group of health care professionals of varied disciplines with knowledge of the complexities related to designing the modern and “smart” intensive care unit (ICU). In this article, we explore the connectivity environment within the ICU, middleware technologies to address a host of patient care initiatives, and the core informatics concepts necessary for both the design and implementation of advanced informatics systems.
Advanced informatics systems can help improve health care delivery and the environment of care for critically ill patients. However, identifying, testing, and deploying advanced informatics systems can be quite challenging. These processes often require involvement from a collaborative group of health care professionals of varied disciplines with knowledge of the complexities related to designing the modern and “smart” intensive care unit (ICU). In this article, we explore the connectivity environment within the ICU, middleware technologies to address a host of patient care initiatives, and the core informatics concepts necessary for both the design and implementation of advanced informatics systems.









 As the world becomes increasingly connected and information is freely shared, a trend toward interdisciplinary collaboration is taking place in both industry and education. This trend is highlighted by recent collaboration between clinicians and architects in both research and design. In the design of healthcare spaces, architects are working with clinicians and researchers to employ an evidence-based approach to making design decisions.
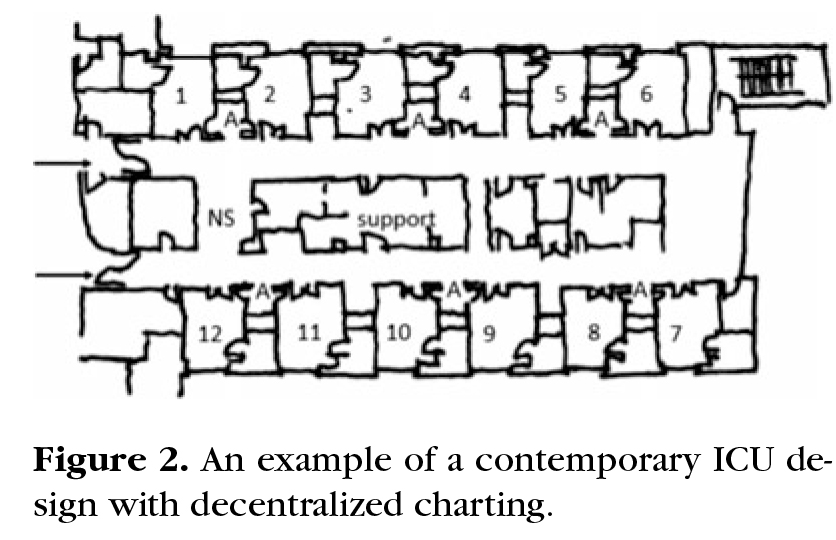
As the world becomes increasingly connected and information is freely shared, a trend toward interdisciplinary collaboration is taking place in both industry and education. This trend is highlighted by recent collaboration between clinicians and architects in both research and design. In the design of healthcare spaces, architects are working with clinicians and researchers to employ an evidence-based approach to making design decisions. Rounding is critical to developing integrated care plans, and there is a trend for moving daily rounds from the bedside to conference rooms. This study’s aim was to document staff preferences for the location of rounding practices, and to determine the effect of available space on those preferences.
Rounding is critical to developing integrated care plans, and there is a trend for moving daily rounds from the bedside to conference rooms. This study’s aim was to document staff preferences for the location of rounding practices, and to determine the effect of available space on those preferences.